

A clinical messaging framework is defined as a structured, HIPAA-compliant system that enables secure, timely, and standardized exchange of clinical information among care teams, patients, and electronic health records. Without one, communication breaks down at the exact moments that matter most. 82% of physicians report that communication fragmentation causes prior authorization delays and treatment abandonment. That single statistic captures the operational and human cost of unstructured clinical communication. The clinical messaging framework explained in this article covers the technical standards, compliance requirements, and practical benefits that healthcare professionals need to implement these systems effectively in 2026.
What are the core technical components of a clinical messaging framework?
A modern healthcare messaging framework is built on HL7 FHIR Release 4, specifically the Communication resource, which organizes messages into a two-level hierarchy. The top level is a thread header that defines the conversation context, participants, and access controls. Each reply or update is a child message linked to that header. This hierarchy supports querying unread threads and routing messages across channels including SMS, in-app chat, and patient portals.
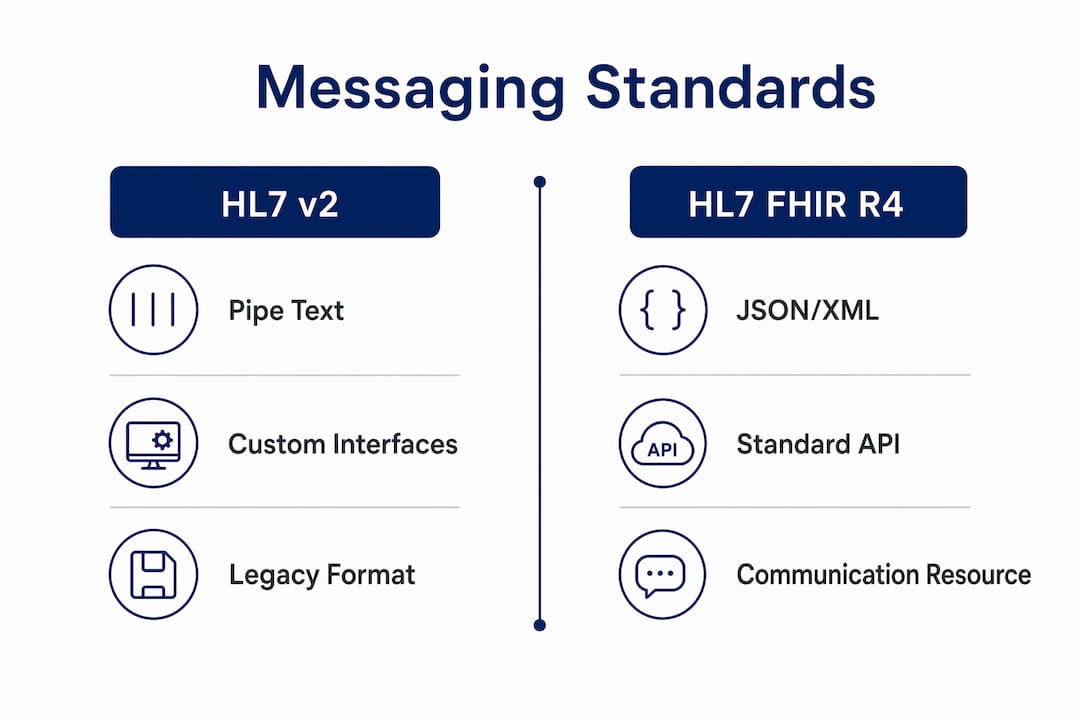
The shift from HL7 v2 to FHIR is not a minor upgrade. HL7 v2 relied on pipe-delimited text segments that required custom parsers and broke frequently across system boundaries. FHIR with JSON-based APIs allows real-time clinical communication and direct connectivity with third-party applications. That means a care coordinator’s message can trigger an alert in a patient’s mobile app and simultaneously update the EHR record, all within a single API call.

SMART on FHIR extends this further by providing a standardized authorization layer. It allows third-party apps to connect to EHR systems without custom integration work for each vendor. Identity resolution and message auditability are built into the FHIR resource model, with each Communication resource carrying sender, recipient, timestamp, and payload fields.
Pro Tip: When evaluating platforms, confirm that the vendor uses FHIR R4 Communication resources natively, not a proprietary data model wrapped in a FHIR-labeled API. The difference matters for long-term interoperability.
One of the most underappreciated technical challenges is external thread matching. When a patient sends an SMS reply, the system must match that inbound message to the correct FHIR thread using an external conversation ID. Using FHIR conditional references and storing external identifiers prevents disconnected messaging and fragmented conversation histories. Without this, a patient’s reply lands in a void, and the care team never sees it.
| Feature | HL7 v2 | HL7 FHIR R4 |
|---|---|---|
| Data format | Pipe-delimited text | JSON or XML |
| Integration method | Point-to-point custom | RESTful API |
| AI and app connectivity | Limited | Native via SMART on FHIR |
| Thread and audit support | Manual | Built into resource model |
| Real-time capability | Batch-oriented | Event-driven |
How does a clinical messaging framework improve patient outcomes?
Structured clinical communication transforms how patients perceive their care team. A 2026 study identified eight distinct empathy communication types that facilitate problem-solving and patient-centered history-taking. That finding matters because empathy is not just a soft skill. It is a measurable communication behavior that standardized messaging protocols can support and reinforce at scale.
The operational benefits are equally concrete:
- Reduced treatment abandonment: Fragmented communication is a direct driver of patients dropping out of care plans. Structured messaging keeps care teams aligned and patients informed.
- Fewer clinical errors: When messages follow a defined format with required fields, critical information is less likely to be omitted or misread.
- Eliminated re-keying costs: Secure messaging eliminates manual re-keying, saving time and reducing transcription errors compared to paper-based or fax workflows.
- Prior authorization support: Structured threads create a documented communication trail that supports prior authorization workflows and reduces back-and-forth with payers.
- Compliance documentation: Every message in a FHIR-native system is a timestamped, auditable record that satisfies documentation requirements across payer and regulatory contexts.
Standardized messaging also changes how patients perceive clinician competence. Structured communication transforms patient perceptions of clinician warmth and professionalism, which directly influences treatment adherence. A patient who feels heard and informed through consistent, well-structured messages is more likely to follow through on a care plan.
The connection between communication quality and clinical outcomes is not theoretical. Care teams that use structured messaging report fewer missed follow-ups, faster response to deteriorating patient conditions, and stronger patient-provider relationships. These are the outcomes that value-based care contracts measure and reward.
What are the compliance requirements for implementing clinical messaging?
Compliance is not a feature you add after deployment. It is the foundation the entire system must be built on. The implementation process follows four non-negotiable steps.
-
Audit existing communication workflows. Map every channel your team currently uses, including personal cell phones, consumer apps, and unencrypted email. Identify where protected health information (PHI) is being transmitted without adequate controls. This audit reveals your actual risk exposure, not your assumed one.
-
Select a platform with encryption at rest and in transit, multi-factor authentication, and role-based access controls. These are baseline requirements, not differentiators. Any platform that cannot confirm all three is not a compliant option.
-
Sign a Business Associate Agreement with every vendor that handles PHI. A signed BAA is non-negotiable for HIPAA compliance. Without it, your organization bears full liability for any breach involving that vendor’s system.
-
Enable granular audit logging. Audit logging must capture message content, user identities, and timestamps to meet HIPAA Security Rule incident response requirements. Logging at the session level is not sufficient. You need message-level records.
Pro Tip: Do not treat the BAA as a checkbox. Review the vendor’s breach notification timelines and subcontractor disclosure requirements before signing. These terms determine your exposure window in a real incident.
Staff training is the step most organizations underestimate. Clinicians need leadership support, protected time, and specific training to integrate structured communication frameworks successfully. A technically compliant platform fails if staff revert to personal devices because the approved system feels slower or harder to use.
What are the common pitfalls in clinical messaging implementation?
The most common mistake is treating a clinical messaging framework as a notification system. Notifications push information in one direction. A true messaging framework manages bidirectional, threaded conversations with access controls, audit trails, and clinical context attached to every exchange. Organizations that deploy notification tools and call them messaging frameworks create a false sense of security.
Several other pitfalls appear consistently across implementations:
- Unresolved sender identity: When a patient replies via SMS, the system must match that reply to the correct provider and thread. Without FHIR conditional references and external conversation ID storage, replies become orphaned records.
- Speed-versus-privacy tradeoffs: Urgent clinical situations create pressure to use whatever channel is fastest. Without clear protocols, clinicians default to consumer messaging apps that offer no PHI protection.
- Neglecting cultural adoption: Technology alone does not change behavior. Organizations that skip change management see low adoption rates within 90 days of go-live, regardless of platform quality.
- Ignoring thread state consistency: A thread that shows as “read” for one provider but “unread” for another creates confusion and missed follow-ups. The two-level FHIR hierarchy must be implemented correctly to maintain state across all users and channels.
- Underestimating training scope: Training cannot be a single onboarding session. Ongoing reinforcement and protocol updates are required as workflows evolve and new staff join.
The organizations that get this right treat messaging implementation as a clinical workflow change, not an IT project. That framing changes who lead the effort, who is accountable, and how success is measured.
Key takeaways
A clinical messaging framework succeeds only when FHIR-native architecture, HIPAA compliance controls, and clinical workflow adoption are addressed together, not in sequence.
| Point | Details |
|---|---|
| FHIR R4 is the standard | Use platforms built natively on HL7 FHIR R4 Communication resources for real interoperability. |
| BAA is non-negotiable | Sign a Business Associate Agreement with every vendor handling PHI before go-live. |
| Audit logging is required | Capture message content, user identities, and timestamps to meet HIPAA Security Rule requirements. |
| Thread matching prevents gaps | Store external conversation IDs to prevent orphaned replies from SMS and other stateless channels. |
| Training drives adoption | Clinicians need protected time and leadership support to integrate structured messaging into daily workflows. |
Why I think most organizations are still getting clinical messaging wrong
I have worked with health systems managing 3,000-plus providers and ACOs covering 375,000 lives. The pattern I see repeatedly is this: organizations invest in the platform and skip the workflow redesign. They buy a FHIR-compatible messaging tool, complete the BAA, enable audit logging, and then wonder why adoption stalls at 40% six months later.
The gap is almost never technical. It is cultural. Clinicians are not resisting the technology. They are resisting the disruption to workflows that were already stretched thin. The fix is not more training sessions. It is leadership that models the behavior, protected time built into schedules, and a clear answer to the question every clinician is silently asking: “How does this make my day easier, not harder?”
FHIR is not just a technical standard. It is the platform on which AI-assisted clinical decision support will run over the next five years. Organizations that adopt FHIR-native messaging now are not just solving a compliance problem. They are building the infrastructure for AI integration that will define competitive advantage in value-based care. The organizations that wait will face a much steeper migration cost later, both technically and culturally.
If you are a healthcare executive or health IT leader evaluating your current communication infrastructure, the question is not whether to move to a structured framework. The question is how fast you can do it without breaking the workflows your clinical teams depend on today.
— Paul
Clinical messaging consulting from Thestartupmd
Implementing a secure, FHIR-native clinical messaging framework requires more than selecting the right platform. It requires aligning technical architecture, compliance controls, and clinical workflows into a system your teams will actually use.
Thestartupmd brings 25-plus years of clinical and executive experience to healthcare organizations navigating this transition. From auditing existing communication gaps to advising on FHIR integration and BAA requirements, the consulting services at Thestartupmd are built for health systems, ACOs, and digital health companies that need a credible medical voice guiding the process. If your current messaging infrastructure is creating compliance risk or slowing care coordination, a focused conversation can clarify your next step.
FAQ
What is a clinical messaging framework?
A clinical messaging framework is a structured, HIPAA-compliant system for secure, standardized exchange of clinical information among providers, patients, and EHRs. It uses defined data models, encryption, and audit controls to protect PHI and support care coordination.
How does HL7 FHIR support clinical messaging?
HL7 FHIR R4 provides the Communication resource model that organizes messages into thread headers and child messages, enabling access control, state management, and real-time API integration across EHRs and third-party applications.
What compliance steps are required for clinical messaging?
The four required steps are auditing existing workflows, selecting an encrypted platform with role-based access, signing a Business Associate Agreement with all PHI-handling vendors, and enabling granular audit logging at the message level.
Why do clinical messaging implementations fail?
Implementations most often fail due to unresolved sender identity in stateless channels like SMS, low clinician adoption from insufficient training, and treating messaging as a notification tool rather than a structured, bidirectional communication system.
What is the benefit of structured clinical communication for patients?
Structured communication improves patient trust, perceived clinician competence, and treatment adherence. A 2026 study identified eight empathy communication types that standardized messaging protocols can support at scale across care teams.
Recommended
- Start Up MD – The Startup MD specializes in elevating small to mid-size healthcare startups by offering a comprehensive suite of services, including an integrated digital marketing strategy with targeted lead generation, engaging content creation (long and short-form videos), and custom website design.
- Home – Copy – Start Up MD
- services – Start Up MD